

I’ve heard some strange and troubling things in my career from clients, and friends about their previous therapists, and a recent example from one middle-aged man that his former therapist didn’t think he was gay because he initiates sex with his wife! It prompted me to ask some of my colleagues about their experiences, and many of their examples alarmed me and redoubled my passion for training therapists to work more effectively with their Gender, Sexuality and Relationship Diverse (GSRD) clients.
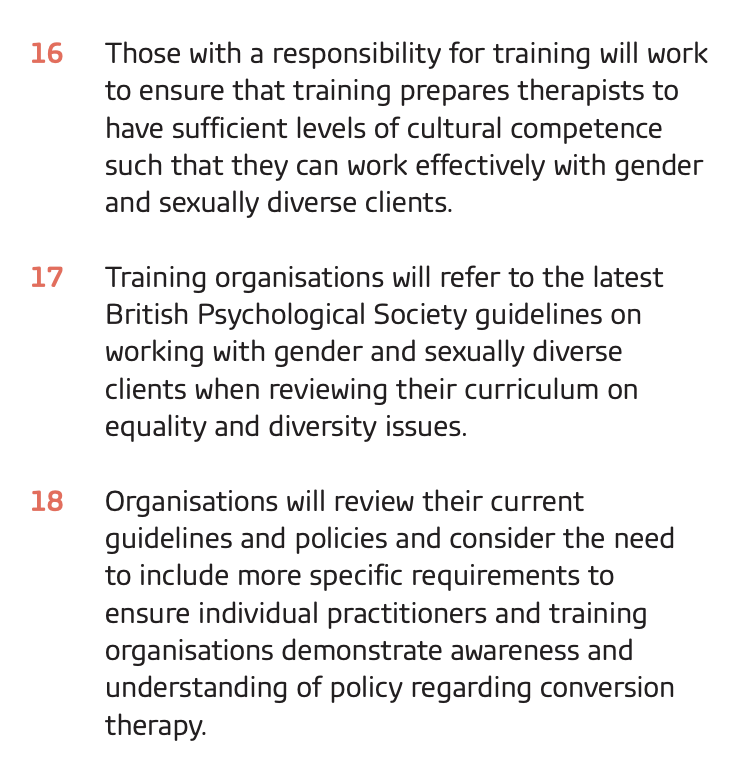
As readers of this blog will know, Pink Therapy has been an active member of a coalition working group of all the leading psy/therapy organisations discussing steps to bring about the end of Conversion Therapy for gender and sexual diversity. The Memorandum of Understanding on Conversion Therapy states:
To this end, we are running running three workshops around the country for therapy trainers to come and share what they’ve already been doing that works well and learn more about a four-stage training model I have developed over my almost 40-year career in delivering training to therapists in this area. We’re holding in London, Manchester and Glasgow because we think face-to-face contact will be more effective at creating the depth of discussion necessary and allowing networks to be built between cisgender heterosexual and LGBT trainers. three, two-day training workshops
But bookings so far have been light. We’ve plastered information all over the Facebook counselling groups, and LinkedIn, we’ve shared the information with the Coalition signatories. The National Counselling Society have told their members and accredited training courses about the workshop. We’ve directly emailed the BACP Accredited courses. I had hoped that by now, the London course would be full, as it is happening in the middle of next month. While we’re oversubscribed on requests from LGBT therapists to attend on training bursaries, so far, very few training courses have decided to send any of their staff (a notable exception being the Contemporary Institute for Clinical Sexology whose Director and GSRD Trainer have been active members on the Coalition working group representing COSRT).
I am still hopeful that we will get some more Counsellor Trainers eager to get a handle on how to embrace the training needs of their students in preparing them to work with GSRD clients, and to share their dilemmas and experience, but if I’m honest, I am not too optimistic.
What do you think is going on? Is it arrogance? Is it cisgender heteronormative prejudice? Is it ignorance? Is it naivety that people don’t know what they don’t know? Or that they don’t think their students need to know very much at all about working with GSRD people as we’re “all the same”? Even as I write this, I am aware it may come across as angry or off-putting. The dilemma of passionately knowing students are being let down, and clients are being harmed whilst trying to encourage those invested in the current system is one which I find myself having to navigate whenever I challenge the status quo.
It’s troubling, and I’m left wondering if we need an independent training route for people who want to specialise in working with GSRD clients because mainstream organisations are failing in their duty of care and responsibilities to prepare therapists adequately. This is something I’ve written about twice before (for Therapy Today and The Psychotherapist). Perhaps we need route that circumvents mainstream Diplomas in Counselling and Psychotherapy. However, given that the core of being person-centred is hope, a belief that positive change can occur, I cannot totally give up on my peers and contemporaries who in colleges, universities and training institutions across the land are educating the next generation of counsellors and psychotherapists. Indeed, I do not want to give up on them, these workshops are designed to support them in their work! Working as I have over the years with so many allies who have devoted their time and energy to improving the LGBT experience, I know that things can improve and have to believe that the GSRD aware trainers course can be part of that positive change and growth.
Dominic Davies
October 2019

 my mind. I am renouncing my Fellowship as I feel incredibly angered by their incompetence and duplicity. I realise this is an empty gesture as probably no-one gives a fuck, not least anyone at BACP, but I feel contaminated by associating my name and reputation with theirs. I’ve had enough of them!
my mind. I am renouncing my Fellowship as I feel incredibly angered by their incompetence and duplicity. I realise this is an empty gesture as probably no-one gives a fuck, not least anyone at BACP, but I feel contaminated by associating my name and reputation with theirs. I’ve had enough of them!
 I am grateful that to everyone who played a part in lobbying the Board with their views, research and concerns. I think this has been immensely helpful in helping the Board decide that these protections are needed.
I am grateful that to everyone who played a part in lobbying the Board with their views, research and concerns. I think this has been immensely helpful in helping the Board decide that these protections are needed.

